Shoulder Specialist in Ahmedabad explains..
Who Is This Article For?
This in-depth clinical guide is intended for:
- Patients experiencing persistent or unexplained shoulder pain
- Individuals with difficulty lifting the arm or weakness
- Athletes and gym-goers with overuse injuries
- Middle-aged and elderly patients with degenerative shoulder symptoms
- Diabetic patients with associated shoulder stiffness
- Anyone trying to differentiate between benign shoulder strain and structural injury
This article is written not just to inform, but to help you make a correct, timely clinical decision.
⚠️ Reality: Why Rotator Cuff Tears Are Frequently Missed
In orthopedic practice, one of the most underdiagnosed conditions is the rotator cuff tear in its early stages.
Most patients present late because:
- Initial symptoms are mild
- Pain is intermittent
- Function is partially preserved
- Symptoms are attributed to “muscle strain”
However, from a pathological standpoint:
👉 A rotator cuff tear is a progressive structural failure, not a temporary inflammation.
The delay between onset and diagnosis often determines:
- Whether treatment remains conservative
- Or progresses to surgical necessity
🦴 Anatomy and Biomechanics of the Rotator Cuff
To understand early symptoms, one must understand the structure.
The rotator cuff comprises four muscles:
- Supraspinatus – initiates abduction
- Infraspinatus – external rotation
- Teres minor – external rotation
- Subscapularis – internal rotation
These tendons converge to stabilize the glenohumeral joint, ensuring dynamic control.
📌 Critical Concept: Force Couple Mechanism
The rotator cuff maintains a balanced force couple, allowing smooth shoulder motion.
When even one tendon is compromised:
- Biomechanics are altered
- Load distribution becomes abnormal
- Progressive degeneration occurs
⚙️ Pathophysiology: How a Tear Develops
Rotator cuff tears are not always sudden events.
🔬 Degenerative Cascade
- Tendon hypovascularity
- Microtrauma accumulation
- Collagen fiber disorganization
- Partial thickness tear
- Full thickness tear
- Retraction and muscle atrophy
⚠️ Important Insight:
👉 Once tendon retraction and fatty infiltration occur, healing potential significantly reduces.
📊 Classification of Rotator Cuff Tears
Each stage correlates with symptom severity—but early symptoms are often subtle.
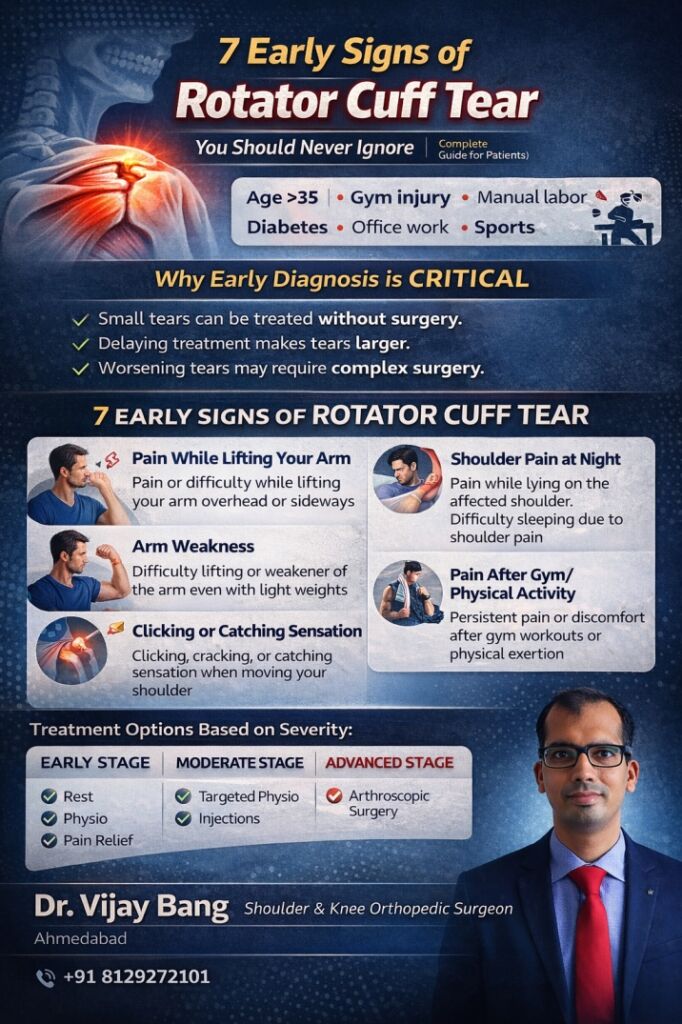
🔥 7 Early Signs of Rotator Cuff Tear (Clinical Expansion)
1. Pain During Active Elevation of the Arm
Clinical Observation:
Pain is typically elicited between 60–120 degrees of abduction (painful arc).
Mechanism:
- Supraspinatus tendon compression under acromion
- Early tendon inflammation or microtear
Clinical Relevance:
Patients often ignore this phase, assuming muscular fatigue.
2. Nocturnal Pain (Night Pain)
Clinical Importance:
Night pain is one of the most predictive symptoms of rotator cuff pathology.
Mechanism:
- Reduced cortical inhibition
- Increased inflammatory mediator activity
- Compression of subacromial space
Red Flag:
👉 Persistent night pain should always raise suspicion of structural pathology rather than simple strain.
3. Early Muscle Weakness
Clinical Finding:
- Weakness in abduction
- Weakness in external rotation
Differentiation:
- Pain inhibition vs true weakness must be clinically distinguished
Key Insight:
👉 Weakness indicates functional compromise of tendon integrity.
4. Activity-Induced Pain (Especially Overhead Use)
Common in:
- Athletes
- Manual laborers
- Gym users
Mechanism:
Repetitive impingement leads to:
- Microtears
- Tendon degeneration
5. Mechanical Symptoms (Clicking, Catching)
Explanation:
- Tendon instability
- Subacromial impingement
- Associated labral pathology
Clinical Tip:
These symptoms often precede significant structural damage.
6. Loss of Functional Internal Rotation
Daily Indicators:
- Difficulty tucking shirt
- Difficulty reaching back pocket
Mechanism:
Subscapularis involvement or altered biomechanics.
7. Progressive Symptom Pattern
Most Critical Sign:
Gradual worsening indicates:
- Tear progression
- Compensatory muscle fatigue
- Joint imbalance
🧪 Clinical Examination vs Self-Assessment
Important Clinical Tests:
- Jobe’s Test
- Drop Arm Test
- External Rotation Lag Sign
Patient-Level Screening:
While home tests can indicate suspicion, definitive diagnosis is clinical.
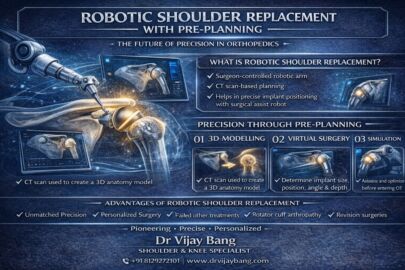
🧠 Imaging Strategy: When MRI Is Justified
MRI Indications:
- Persistent symptoms > 6 weeks
- Suspected full-thickness tear
- Preoperative planning
Clinical Principle:
👉 Treat the patient, not the MRI report.
💊 Management Strategy Based on Stage
Stage 1: Early / Inflammatory Phase
- Activity modification
- NSAIDs
- Structured physiotherapy
Stage 2: Partial Tear
- Rotator cuff strengthening
- Scapular stabilization
- Injection therapy (select cases)
Stage 3: Full Thickness Tear
- Arthroscopic repair (indicated in active patients)
Stage 4: Chronic / Massive Tear
- Complex reconstruction
- Possible tendon transfer or reverse arthroplasty
🏋️ Rehabilitation Principles
- Early controlled mobilization
- Avoid painful arc overload
- Focus on scapular mechanics
- Progressive resistance training
❌ Clinical Errors Commonly Seen
- Over-reliance on painkillers
- Ignoring weakness
- Continuing aggravating activities
- Delayed referral
- Misdiagnosis as frozen shoulder
⏳ Natural History Without Treatment
Untreated tears may lead to:
- Tear enlargement
- Muscle atrophy
- Fatty infiltration
- Irreversibility
🏥 Why Choose Dr Vijay Bang
- Dedicated shoulder practice
- Expertise in arthroscopic repair
- Evidence-based management
- Focus on early diagnosis
❓ Frequently Asked Questions
1. Can a rotator cuff tear remain asymptomatic?
Yes, especially in early or degenerative tears, patients may not experience significant symptoms initially. However, asymptomatic tears can still progress structurally over time. Studies have shown that untreated tears often enlarge, even in the absence of pain. This silent progression makes early detection challenging. Periodic clinical evaluation is advisable in high-risk individuals.
2. What differentiates pain inhibition from true weakness?
Pain inhibition occurs when muscle contraction is limited due to discomfort, whereas true weakness indicates mechanical failure of the tendon. Clinically, this distinction is made through specific resisted tests. True weakness persists even after pain control measures. Identifying this difference is crucial in decision-making. It often determines whether imaging or surgical intervention is needed.
3. Are degenerative tears inevitable with aging?
While tendon degeneration increases with age, not all individuals develop symptomatic tears. Genetic factors, activity level, and vascular supply influence progression. Preventive strengthening and avoiding repetitive overload can reduce risk. Early symptoms should not be dismissed as “age-related.” Active management improves outcomes significantly.
4. What role does physiotherapy play in tendon healing?
Physiotherapy does not “heal” the tear structurally but improves function by strengthening compensatory muscles. It enhances joint stability and reduces pain. In partial tears, it can significantly delay or avoid surgery. However, compliance and correct technique are essential. Improper rehabilitation can worsen symptoms.
5. When does a tear become irreparable?
A tear becomes irreparable when there is:
- Significant tendon retraction
- Muscle atrophy
- Fatty degeneration
At this stage, direct repair is not feasible. Advanced procedures may be required. Early intervention prevents this progression.
6. Is early surgery better than delayed surgery?
In selected patients (young, active, large tears), early surgery provides better outcomes. Delay can lead to tissue degeneration. However, not all tears require surgery. Decision must be individualized. Clinical judgment is key.
7. Can rotator cuff tear mimic frozen shoulder?
Yes, especially when pain limits movement. However, passive motion remains relatively preserved in cuff tears. Frozen shoulder restricts both active and passive movement. Proper examination differentiates the two.
8. What is the success rate of arthroscopic repair?
Success rates are generally high (80–90%) in appropriately selected patients. Outcome depends on tear size, chronicity, and rehabilitation compliance. Early surgery improves prognosis. Postoperative physiotherapy is crucial.
📢 Final Clinical Takeaway
Rotator cuff tears are:
- Progressive
- Often underdiagnosed early
- Potentially reversible if detected early
👉 Recognizing early signs is not just helpful—it is clinically critical.
📍 Consultation & Contact
Dr Vijay Bang
Shoulder Orthopedic Surgeon in Ahmedabad
www.drvijaybang.com
Call/whatsapp – +91 8129272101
(share your report on WhatsApp for trustable honest opinion)
🔗 Stay Connected with Dr. Vijay Bang for Regular Health Tips:
Instagram: https://www.instagram.com/drvijaybangortho
YouTube: https://www.youtube.com/@drvijaybangortho
Facebook: https://www.facebook.com/drvijaybangortho
Linkedin: https://www.linkedin.com/in/drvijaybangortho/
🔑 Keywords
early signs of rotator cuff tear, rotator cuff tear symptoms early, shoulder weakness causes, rotator cuff tear diagnosis India, shoulder pain specialist Ahmedabad, rotator cuff tear treatment options, when to get MRI shoulder